717
Views & Citations10
Likes & Shares
Background: Microbiological
confirmation of Mycobacterium tuberculosis disease can be challenging in
patients with a low bacterial load or in those who do not expectorate. In such
situations sampling through brochoalveolar lavage (BAL), induced sputum and
gastric lavage are alternatives. The Xpert MTB/RIF assay is a rapid technique
with high sensitivity and specificity for diagnosing TB and detecting drug
resistance in extra pulmonary and smear-negative TB cases and from
Bronchoalveolar lavage. Hence we conducted this study to evaluate the
significance of Xpert MTB/RIF performed on bronchial washing fluid obtained
bronchoscopically from patients with a clinical and radiological suspicion of
pulmonary tuberculosis.
Methods: We retrospectively
reviewed the clinical records and fibre optic bronchoscope (FOB) results of all
patients with suspected PTB who visited the pulmonary clinic of Government
Rajaji Hospital (GRH), Madurai from January 2017 to June 2017.
Results: A total of 100
sputum smear-negative patients were posted for FOB, 71 men (71%) and 29 women
(29%), the median age was 53 years. The patients aged 41 to 60 years (53.5%)
were the ages most frequently encountered. Twenty two out of the 100 BAL
specimens (22.7%) were positive culture for M. tuberculosis by Xpert MTB/RIF.
Drug sensitivity test showed one case (4.5%) resistant to Rifamycin who was
referred to initiate on Multi-drug resistant TB treatment.
Conclusion: This study
revealed high positive rates of PTB from bronchoscopy samples, providing rapid
and definitive ability for PTB diagnosis, and details of drug susceptibility.
Therefore, FOB is an important diagnostic procedure in patients with suspected
PTB whose sputum specimens were negative.
Keywords: Pulmonary
tuberculosis, Fibreoptic bronchoscopy, Xpert MTB/RIF
INTRODUCTION
Too many people have undetected Tuberculosis (TB) for too long; late
detection of TB increases their risk of transmitting the disease to others.
Detecting patients with active Pulmonary Tuberculosis (PT) disease is an
important component of tuberculosis control programs, as early diagnosis and
treatment of pulmonary tuberculosis is essential in reducing the morbidity,
mortality and the escalating costs associated with advanced disease. A high-quality
laboratory system that uses modern diagnostics is a prerequisite for the early,
rapid and accurate detection of TB and drug resistance. In December 2010,
GeneXpert MTB/RIF assay was endorsed by World Health Organisation (WHO) and
then recommended for detection of Mycobacterium tuberculosis (M.TB) complex and
rifampicin resistance [1].
The Xpert MTB/RIF
assay is a rapid and simple technique with high sensitivity and specificity for
diagnosing TB and detecting drug resistance in extra pulmonary and
smear-negative TB cases [3] and from Bronchoalveolar lavage [4,5]. With the
advent of fibre-optic bronchoscopy, smear and culture for mycobacteria from the
bronchial aspirate, bronchial brushing, bronchial washing, bronchoalveolar
lavage fluid, post bronchoscopy sputum and biopsy material have all been used
in various studies for diagnosing pulmonary tuberculosis. There are limited
studies to demonstrate the use of Xpert MTB/RIF performed on bronchial lavage
specimens in our settings. Hence we conducted this study to evaluate the
significance of Xpert MTB/RIF performed on bronchial washing fluid obtained
bronchoscopically from patients with a clinical and radiological suspicion of
pulmonary tuberculosis.
METHODS
Study population
We retrospectively
reviewed the clinical records and fibre optic bronchoscope (FOB) results of all
patients with suspected PTB who visited the pulmonary clinic of Government
Rajaji Hospital (GRH), Madurai from January 2017 to June 2017.
For the purposes of
our study we considered a clinical suspicion of pulmonary tuberculosis if any
two of the following were present: known HIV infection, persistent cough
lasting >3 weeks, hemoptysis, weight loss >4 kg, intermittent fever >3
weeks or drenching night sweats >2 weeks. In addition, at least one of the
following radiological criteria had to be present for inclusion: cavitation,
diffuse infiltrates, hilar or mediastinal adenopathy. All had 2 early morning
sputum smears negative for AFB by fluorescent microscope stain. They had no
response to 2 weeks antibiotics used for lower respiratory tract infection. The
study was approved by the Hospital Ethics Committee. A waiver of consent was
obtained due to the retrospective nature of the study.
Procedure
Bronchoscopic
procedure was performed according to our institute’s infection regulation and
instruction guideline. The patients were informed about the procedure and
consents were obtained. The patients underwent bronchoscopy by flexible
fiberoptic bronchoscope through trans nasal route in supine position and under
local anaesthesia. All the patients underwent continuous monitoring of
electrocardiogram, blood pressure and pulse oximetry. After inspection of the
bronchial tree, BAL was done with 100 ml of normal saline at the end of
bronchoscopy in the region suspected for lesion based on chest radiography. The
patients were observed in the recovery room. BAL samples were sent for
fluorescent microscope stain, fungal smear, and cytopathology. Proper disinfection
of the bronchoscope in between use was done. All Xpert MTB/RIF samples were
processed according to the manufacturer’s specifications.
RESULTS
All the records were
scrutinized, checked and computerized by trained data entry operators. Data
entry was done in Excel 2013 and analysis was performed using SPSS 20.
Descriptive statistics were performed. The study involved the patients
attending the TB clinic in GRH, who had clinical and radiological findings
suggestive for PTB, whose sputum smear were negative by fluorescent microscopy
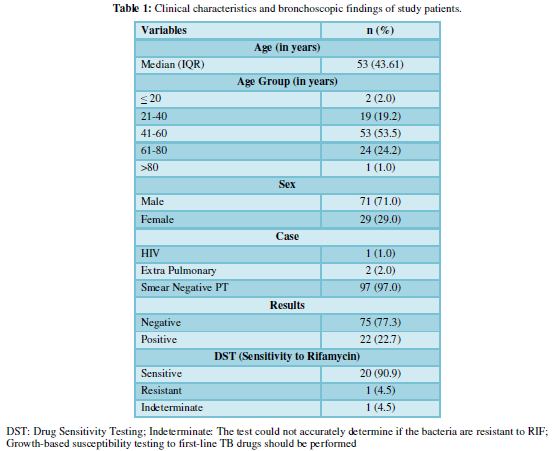
and a FBO was performed for TB diagnosis. A total of 100 sputum smear-negative
patients were posted for FOB, 71 men (71%) and 29 women (29%), the median age
was 53 years. The patients aged 41 to 60 years (53.5%) were the ages most
frequently encountered (Table 1).
Twenty two out of the 100 BAL specimens (22.7%) were positive culture for M. tuberculosis by Xpert MTB/RIF. Drug
sensitivity test showed one case (4.5%) resistant to Rifamycin who was referred
to initiate on multi-drug resistant TB treatment.
DISCUSSION
Fiberoptic
bronchoscopy (FOB) is an alternative option to provide respiratory specimens
for diagnosis, particularly from sites which are suspected by radiological
findings to be involved in PTB after sputum expectoration has continually
failed because of lacking sputum. We evaluated the clinical value of Xpert
MTB/RIF assays for the diagnosis of active PTB in sputum-scarce PTB suspects in
TB endemic setting.
In our study bronchial
washings Xpert was positive for acid fast bacilli in 22.7% patients which were
missed in smear microscopy. Although sputum microscopy is the most appropriate,
low cost, highly specific investigation to diagnose pulmonary tuberculosis,
Sputum smear-negative pulmonary tuberculosis (SSN-PTB) still remains a common
problem faced by the clinicians. Despite being less infectious than sputum
smear-positive PTB, smear-negative PTB serves as an important cause of
transmission in communities by delaying diagnosis and precluding initiation of
treatment and often leads to complications of irreversible lung damage in
infected individuals. Diagnosis of sputum smear-negative pulmonary tuberculosis
patients can be both challenging and time consuming with many patients being
put on empirical anti-tubercular treatment. Therefore, sputum smear-negative
PTB often requires more invasive diagnostic tools to be distinguished from
other diseases such as lung cancer. Fibreoptic bronchoscopy may provide a
Fiberoptic
bronchoscopy (FOB) is an alternative option to provide respiratory specimens
for diagnosis, particularly from sites which are suspected by radiological
findings to be involved in PTB after sputum expectoration has continually
failed because of lacking sputum. We evaluated the clinical value of Xpert
MTB/RIF assays for the diagnosis of active PTB in sputum-scarce PTB suspects in
TB endemic setting.
In our study bronchial
washings Xpert was positive for acid fast bacilli in 22.7% patients which were
missed in smear microscopy. Although sputum microscopy is the most appropriate,
low cost, highly specific investigation to diagnose pulmonary tuberculosis,
Sputum smear-negative pulmonary tuberculosis (SSN-PTB) still remains a common
problem faced by the clinicians. Despite being less infectious than sputum
smear-positive PTB, smear-negative PTB serves as an important cause of
transmission in communities by delaying diagnosis and precluding initiation of
treatment and often leads to complications of irreversible lung damage in
infected individuals. Diagnosis of sputum smear-negative pulmonary tuberculosis
patients can be both challenging and time consuming with many patients being
put on empirical anti-tubercular treatment. Therefore, sputum smear-negative
PTB often requires more invasive diagnostic tools to be distinguished from
other diseases such as lung cancer. Fibreoptic bronchoscopy may provide a
confirmative and early diagnosis in such patients [6].
There are several
limitations in this study. First, it was a retrospective study and the study
population and clinical setting were selective, so it is difficult to
generalize this result to other settings. Second, to improve diagnostic
accuracy and ensure safety, a well-trained pulmonologist is essential for the
use of FOB in the diagnosis of PTB.
This study revealed
high positive rates of PTB from bronchoscopy samples, providing rapid and
definitive ability for PTB diagnosis and details of drug susceptibility.
Therefore, FOB is an important diagnostic procedure in patients with suspected
PTB whose sputum specimens were negative.
ACKNOWLEDGEMENT
We would like to thank
the Institute for permitting us to utilise the Hospital medical records of the
patients. We also thank Ms. Kayalvizhi and Ms. Gomathi for assisting in data
collection.
AUTHORS CONTRIBUTION
1. World Health Organization (2014) Companion
handbook to the WHO guidelines for the programmatic management of
drug-resistant tuberculosis.
2. Brown M, Varia H, Bassett P, Davidson RN,
Wall R, et al. (2007) Prospective Study of sputum induction, gastric washing
and bronchoalveolar lavage for the diagnosis of pulmonary tuberculosis in
patients who are unable to expectorate. Clin Infect Dis 44: 1415-1420.
3. Ullah I, Javaid A, Masud H, Ali M, Basit A,
et al. (2017) Rapid detection of Mycobacterium tuberculosis and rifampicin
resistance in extrapulmonary tuberculosis and sputum smear-negative pulmonary
suspects using Xpert MTB/RIF. J Med Microbiol 66: 412-418.
4. Khalil KF, Butt T (2015) Diagnostic yield of
bronchoalveolar lavage gene Xpert in smear-negative and sputum-scarce pulmonary
tuberculosis. J Coll Physicians Surg Pak 25: 115-118.
5. Barnard DA, Irusen EM, Bruwer JW, Plekker D,
Whitelaw AC, et al. (2015) The utility of Xpert MTB/RIF performed on bronchial
washings obtained in patients with suspected pulmonary tuberculosis in a high
prevalence setting. BMC Pulm Med 5: 103.
6. Arshad AB, Rahul G, Inaamul H, Hanumant GV
(2010) Diagnosing sputum/smear-negative pulmonary tuberculosis: Does
fibre-optic bronchoscopy play a significant role? Lung India 27: 58-62.
7. Menon PR, Lodha R, Singh U, Kabra SK (2011) A
prospective assessment of the role of bronchoscopy and bronchoalveolar lavage
in evaluation of children with pulmonary tuberculosis. J Trop Pediatr 57:
363-367.
8. Sinha S, Guleria R, Pande JN, Pandey RM
(2004) Bronchoscopy in adults at a tertiary care centre: Indications and
complications. J Indian Med Assoc 102: 152-156.
-
 Table 1
Table 1
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Chemotherapy Research Journal (ISSN:2642-0236)
- Advance Research on Alzheimers and Parkinsons Disease
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)


